
Mirrors and Memories
How they erased a season — and how I remembered it anyway.

Mirrors and Memories
Aug 8, 2025
How they erased a season — and how I remembered it anyway.

I woke up this morning at 3 a.m. as usual. The sound of crickets near and far was like a symphony, the wind brushing over the silhouette of treetop shadows and faint, clouded moonlight. It’s been such a foggy summer this year — a haze has been present every day, even in pictures. I don’t recall a summer where there has been such a permanent haze.
In my inner world, I’m still staring at the same haze. Maybe that’s why I notice it so much in the outer. I’m still stuck in a memory loop of solitary confinement and gaslighting. I can see through memory with a dexterity and objectivity — like the early morning canvas out my window. Time stands still. It’s not linear; it moves back and forth like the wind. And yet the present moment is like holding water with cupped hands.
There’s a mirror in every hospital, but not for the patient. The real mirrors are the professionals — cold, indirect, and distorted. You learn to read them, not for truth, but for survival. And if you manage to escape, the real process begins: remembering what you saw in them — and what they refused to see in you.
The stories I’ve written aren’t about a singular moment of mistreatment. They were all meant to place memories on a shelf like a book, and walk away just knowing they happened. So they’re not burned or rewritten should I turn away. But what happens after?
Healing and justice can’t be tied together — I’ve learned that this summer. Only healing — and personal accountability for seeing things clearly as they truly are — seems to facilitate that.
What has happened after: the bureaucratic fog, the search engine suppression, the information wars, the silence. It’s about how a person — stripped of agency and then voice — is expected to thank the system for not being worse.
Since March 2025, I’ve lived inside a process. It was meant to protect patients, hold doctors accountable, and allow truth to surface. That process is called the CPSO and HRTO complaints systems. There was even a patient advocate at one time. But like the rest, he disappeared into silence. What I’ve learned is that these are not mechanisms for truth. They appear to be containment strategies.
You see, when I was released by Tribunal from North Bay Regional Health Centre, I believed that recovery meant proving what happened: the myriad of laws broken, the malpractice, the outright cruelty. The B52 injections. The gaslighting. The solitary confinement. The falsified records. The trauma mischaracterized as pathology. I believed that if I could lay it all out — legally, coherently, truthfully — someone would step in. That illusion didn’t last.
Three months. Hundreds of pages of records. A forensic exhibit. An evidence matrix outlining legal violations. Rebuttals, timelines, affidavits of experience. None of it seemed to matter to the institutions. Their representatives rotated as though the purpose of the investigation was to determine how much credible information the patient had, not whether misconduct occurred.
And while I wrote, they scrubbed. Bing stopped returning results. Images vanished. I watched as my stories were suppressed, then resurgent, then suppressed again. But Google — Google held the line. I was number 2 under Parker’s license number. Number 6 under her full name. The truth found its cracks in the algorithm.
But what no algorithm can restore is a lost summer. A season where I couldn’t garden. Couldn’t build. Couldn’t connect. Trauma recall consumed the hours. Writing became the only coherent act. Medium became the only platform that let me speak without interruption.
No psychiatrist checked in. The one who knew me for years went silent. Parker erased me, and no one contested it. That’s what I mean by mirrors. These professionals reflected back nothing but what they’d already decided. And that’s what I mean by memories. I kept them all.
This isn’t just about me. It’s about what happens when a system turns a patient into a case file, a security threat, a pathology. And what happens when that patient outlives the label — and starts talking.
I’m grateful to Medium for allowing my memories to be more than internal burdens. Here, they are public record.
No one can erase that now.
I’ve learned that even if you have clear evidence of human rights violations and malpractice — and expose them directly, publicly, and simply ask for correction to literal laws broken — there is still no accountability. No one cares. No one is supposed to see. It’s easier to suppress my stories than acknowledge the laws that were broken.
This summer taught me that healing cannot be tied to justice — even if it is technically achievable, even if I can see its shadow over the treetops for myself and others. Even if the good that could come of it by means of reform will probably serve to intensify their protocols and erase minds with traumatic experience even more completely.
Survival is such a curious thing.
What I began to feel, long after the sedation wore off and the documentation took shape, was not their remorse — but their discomfort. It wasn’t guilt that stalked the halls after exposure, but the loss of a closed-stage performance. Their cruelty, perfected over time, had always relied on secrecy and internal applause. They mocked, subdued, erased — all with the silent assumption of impunity. But I changed the lighting. I opened the door. Now every smirk, every omission, every taunt lives under possible observation. The audience expanded. And they can feel it. It wasn’t regret. It was the grief of losing control over their narrative.
Postscript for Donors and Institutional Memory
While no public response was offered to the forensic evidence submitted — first to the hospital’s patient advocate, then to the Ontario Ombudsman, then circled back again, and finally escalated to the CPSO and HRTO — no rebuttal was received to the legal matrix of violations presented. What followed was not engagement, but erasure.
Estimated institutional cost of formally rebutting a legally structured forensic exhibit across four oversight bodies: between $35,000 and $75,000, including legal counsel review, internal compliance vetting, risk exposure analysis, and coordinated communication response.
Estimated monthly cost of third-party suppression services (including reputation management, search engine suppression, SEO flooding, and public relations monitoring): $10,000–$20,000/month, with ongoing costs compounding across multiple platforms. Suppression campaigns of this scale are typically conducted through private firms, involving tailored media obfuscation and algorithmic de-ranking. Content related to the author was removed or de-ranked, while unrelated institutional material became more prominent in its place.
Across a 3-month suppression window, this represents a probable outlay of $60,000 or more — spent not on resolution, reparation, or trauma-informed policy reform, but on digital scrubbing and silence.
No funds appeared to be allocated toward harm acknowledgment, direct communication, or even a basic reply.
For those who donate to North Bay Regional Health Centre, this may raise a question worth asking:
Was your gift used to protect care — or to protect the institution from the consequences of its own conduct?
Postscript — Observational Note. These remarks are made from the standpoint of lived experience and not as formal accusations toward any individual.
(Filed for public awareness and institutional learning purposes)
In the course of this matter, it has become apparent that certain institutional environments can develop cultures where patient interactions are not only clinical but may also carry entertainment value for staff. This observation is not intended as an accusation toward any specific person or body, but as an acknowledgment that in some high-stress care settings, a combination of sociopathic and psychopathic traits may be present among team members.
While such traits can be advantageous in environments requiring detachment, they may also influence the way patient distress is perceived or responded to. The result, for some patients, is the experience of being part of a performance rather than a therapeutic process. This dynamic, though rarely acknowledged, may be sustained by oversight systems whose procedural mandates inadvertently shield the institution as a whole.
This note is offered not as criticism but as clarification for those who assume that all clinical encounters are purely therapeutic. It is also an apology to anyone unfamiliar with such realities, for disclosing a perspective that may alter how they view certain professional environments.
I Was Drugged Before I Was Diagnosed:
A Forensic Case Study of Involuntary Psychiatry at North Bay Regional Health Centre (NBRHC)
📜 Disclaimer
This article reflects the personal lived experience, interpretations, and opinions of the author. All statements concerning Dr. Vivien Mary Parker (CPSO#: 68883), North Bay Regional Health Centre, and other named individuals or institutions are based on documented personal medical records, direct observation, and materials disclosed during active legal and regulatory proceedings. The author makes no allegation of criminal behavior, but asserts their right to critique medical conduct, institutional accountability, and psychiatric practices as matters of public interest, protected under the Canadian Charter of Rights and Freedoms and applicable fair comment doctrine. All statistical modeling presented is hypothetical and provided for illustrative purposes only.
“All interpretations are personal and based on my lived experience under sedation and extreme stress. I recognize that other interpretations may exist.”
“All references to medical professionals are made in the context of public accountability and are not intended to defame character or question competency outside of the documented experience.”
At the time of publication, the matters described remain under review by the College of Physicians and Surgeons of Ontario (CPSO) and the Human Rights Tribunal of Ontario (HRTO). All conclusions and probability estimates presented herein reflect the author’s personal interpretation of documented events and may be updated in light of future rulings. They are not findings or determinations made by any regulatory or legal authority.
Addendum to Mirrors and Memories: Standard Operating Procedure (SOP)
August 2025
This amendment is written in good faith, without hostility, and in service of clarity. It is offered to accompany the narrative of Mirrors and Memories, not to accuse, but to articulate what has been observed repeatedly during and after involuntary psychiatric detainment.
After extensive documentation, testimony, and cross-referenced evidence were submitted to the College of Physicians and Surgeons of Ontario (CPSO), the Human Rights Tribunal of Ontario (HRTO), and the North Bay Regional Health Centre (NBRHC), the following procedural pattern has been identified. The examples cited reflect documented experiences in the author’s own case and recurring elements described in other public or investigatory records.
Standard Operating Procedure (SOP)
Step 1: Containment
Rapid sedation initiated before a formal psychiatric diagnosis. No emergency declared or consent given. Resistance or questioning is pathologized.
Form 1 certification filled out late or retroactively.
Forms 3, 33, and 50 signed while the patient is chemically sedated.
Observation protocols used to justify prolonged solitary confinement.
Step 2: Narrative Construction
Staff provoke or escalate, then document reactions without context.
Trauma responses are labeled as pathology.
Humour, warmth, or noncompliance is recorded as instability.
Accurate patient self-reporting is dismissed.
Step 3: Communication Control
Legal counsel delayed until after sedation.
Phone access tightly monitored or restricted.
Patient advocacy efforts redirected or neutralized.
Staff claim “the patient chose not to attend” key hearings.
Step 4: Exit Without Accountability
Once tribunal releases the patient, no follow-up is offered.
Medical records are left incomplete or contradictory.
CPSO and HRTO responses rely on procedure, not substance.
Witnesses within the institution close ranks or are reassigned.
Step 5: Suppression & Surveillance
Public search results are suppressed or manipulated.
No staff are held accountable.
Patient stories are dismissed as isolated incidents or pathology.
When undeniable, silence is used to smother visibility.
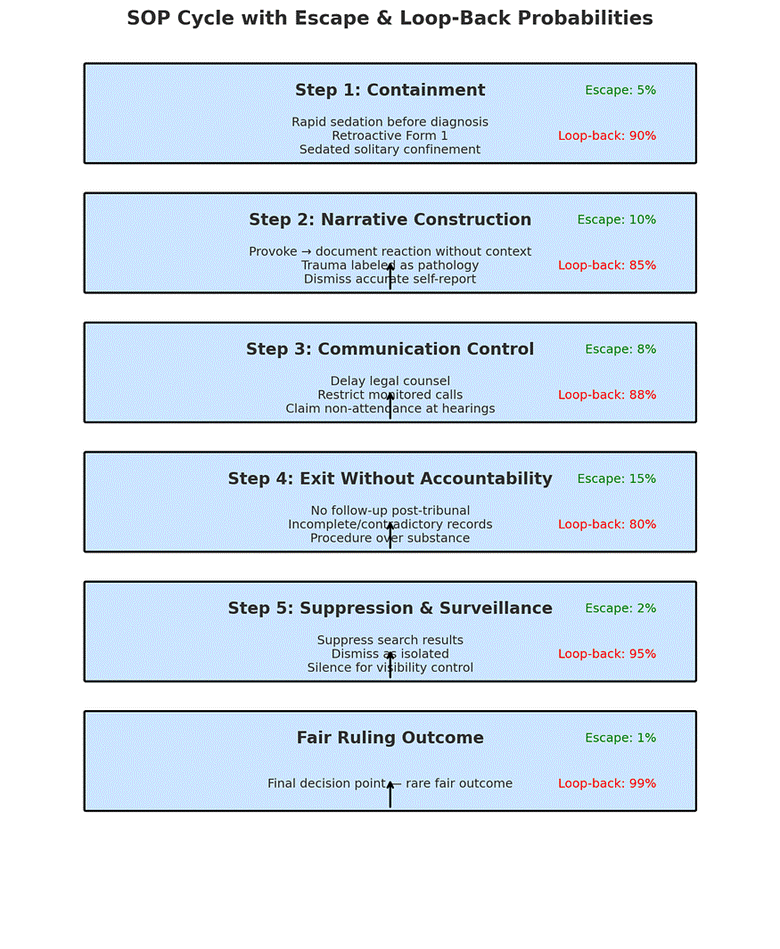
SOP Cycle Probabilities (Illustrative Only)
The following figures are illustrative, based on the author’s interpretation of available documentation, and are not empirical data:
● Containment: Escape probability ~5%; Loop-back ~90% (back to Containment if deemed “escalating” or “noncompliant”).
● Narrative Construction: Escape ~15%; Loop-back ~70% (provoked reaction reframed as instability → renewed sedation/solitary).
● Communication Control: Escape ~20%; Loop-back ~65% (counsel delayed or contact restricted → back to earlier stages).
● Exit Without Accountability: Escape ~40%; Loop-back ~50% (post-release investigation triggers re-engagement with system).
● Suppression & Surveillance: Escape ~60% (with independent platforms); Loop-back ~30% (smear campaigns or formal responses).
● End-State: Probability of fair ruling (CPSO/HRTO) ~5–10%; Permanent escape without retaliation ~15%; Loop-back into system ~80–85%.
The purpose of publishing this SOP is not retaliation. It is preservation — of memory, truth, and an accurate record of what can occur when trauma meets bureaucracy.
Despite all efforts to the contrary, the stories survived. And so did the author.
This SOP, like the stories it accompanies, is now part of the public record.
Press enter or click to view image in full size
illustrative only
Press enter or click to view image in full size

illustrative only
These illustrative probabilities are metaphorical models created by the author to represent the perceived dynamics within institutional settings.
This article is written in good faith and does not assert any final conclusions of law or liability. It represents the author’s personal interpretation of lived events and documented experience, submitted for public awareness and transparency.
Case References for Transparency
The experiences and findings documented in this narrative remain under formal review at the time of publication. These references are provided solely for the purpose of public accountability and transparency:
• Human Rights Tribunal of Ontario (HRTO) — Case #: 2025–61450-I
• College of Physicians and Surgeons of Ontario (CPSO) — File #: CAS-485715-F3T5Z0
Inclusion of these references does not imply endorsement, validation, or final rulings by either institution.🗂️ Public Archive Index
All articles, evidence, timelines, and formal submissions are indexed here:
https://docs.google.com/document/d/1OBQkZ-kHVA6pr_bRoXP2rOTQKQk2rp7NJmBGzwswSsU/edit?usp=drive_link
his doesn’t read like a complaint — it reads like a field manual smuggled out of captivity. You mapped the cycle step by step, the way only someone who lived it could. It’s chilling not because it’s angry but because it’s procedural. Thank you for refusing to let them turn your memory into their silence
Thank you so much for seeing it as it is and taking the time to express it.